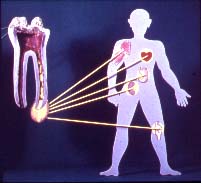
To understand the challenge of
root canal therapy, it is necessary to undertand
the complexity of tooth anatomy. Because the root
of a healthy tooth is made of a highly porous
material which oozes fluids constantly when the
tooth is alive, there is presently no known
technique that can guarantee the total cleaning
and sealing of the entire canal system of a dead
tooth. Furthermore if the tooth is infected, it
is impossible to totally eliminate the infection
so root canal therapy can only reduce, as much as
possible, the amount of infection in the dead
tooth. An infected tooth is thus a more complex
problem then it may seem at first glance. A dead
tooth, root filled or not, is not a healthy
tooth. Even in the absence of infection, the
total lack of dentinal fluid transport means that the tooth is
always vulnerable to microbial invasion.
Studies
have also demonstrated that bacteria can actually
mutate during their life cycle to undergo a quick
"identity change" in order to resist
the effects of antibiotics.
The
above can be summarized by the following quote:
" Root
canal procedures present numerous challenges due
to the porous nature of the root structure and
ease of penetration of microbes inside that
porous structure once the tooth is dead and
deprived of blood supply. Currently it is
impossible to completely clean the entire canal
system of a tooth. If a dead tooth is infected,
it can only be attempted to reduce infection as
much as possible within the limitations of
present treatment modalities. "
Redoing
an existing endodontic treatment is a possible
option that may assist in
further reducing the amount of residual infection
in a tooth, however it is important to be aware
of the limitations, taking into account the
information provided in the previous section on
the challenges of endodontic therapy. The
ultimate success rate in getting rid of
infected/necrotic tissue in the entire canal
system of a tooth will depend on the ability to
fully access the dentinal tubules. If the
previous endodontic treatment was performed with root canal sealers that are insoluble
and/or very difficult to remove and designed to seal the
internal opening of the dentinal tubules, it will be very
difficult, if possible at all, to get good access
to all the dentinal tubules using the
photoacoustic effect.
Without good
access to the dentinal tubules it will not be
possible to clean them or seal them using the
laser assisted ocalexic procedure explained
below.
Each situation
will vary according to the condition of the
tooth, the amount of infection and the type of
materials used by the dentist who performed the
original endodontic treatment.
LASER
ASSISTED OCALEXIC ENDODONTICS
The laser assisted ocalexic
modality is an alternative solution to the
complex challenge of the root canal system. This
treatment protocol goes two steps further than
the conventional root canal therapy by more
effectively targeting the dentinal tubules using 2
key effects:
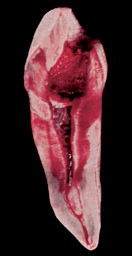
The cross section
photograph of a premolar on the left
shows the calcium oxide in the ocalexic
material that has been absorbed in the
tooth structure. In this special staining
technique it reacts with a
phenolphthalein alcohol solution which
acts as a red marker, proving the
penetration of the inaccessible canals
and dentinal tubules. ( From
Rubrigraphies Ocalexiques - Collection du
Service de Recherches Endodontiques de
l'Ecole Dentaire de Paris )
Usually the
ocalexic root canal treatment will take
the same number of visits as the
conventional root canal treatment. Once
completed the treated tooth must be
monitored to verify the presence or
absence of residual infection. This
verification should not be limited to
clinical ( symptomatology ) and
radiographic assessment since these usual
modalities may not be sensitive enough to
detect chronic infection inside the
dentinal tubules.
As with any treament modality,
success cannot be guaranteed. If chronic
infection persist, further treatment to eliminate
the infection will be recommended since it is
never a good idea to allow a chronic infection to
fester in your body.
If
you need a root canal, talk to our staff to learn
more about ocalexic root canal therapy and other
therapeutic options available because more
than the tooth may be at stake.